Role of ayurveda in the management of female infertility due to pcos with a history of bilateral ectopic pregnancy and right sided salpingectomy & left sided hydrosalpinx.
A clinical case report
ABSTRACT
PCOS, Fallopian Tubal Blockage, Repeated Spontaneous Abortions are some of the causes of female infertility. Hormonal treatment or drilling of ovaries, micro-surgery of fallopian tubes, IVF are some of the treatment. In Ayurveda it is named as Vandhyatva. Garbhasrava, Beeja Dushti and Mithya Ahara Vihara are some of the causes mentioned by our Acharyas. We are reporting a case of infertility due to PCOS with a surgical history of emergency laparoscopic right sided salpingectomy for ectopic pregnancy. And medical history of tab methotrixate for left side ectopic pregnancy, consequently for second time & left sided hydrosalpinx. As per the classical reference treatment was planned for four- karma (virechana karma, kala basthi and marsha nasya karma, and Uttara basthi karma) along with music therapy and yoga chikitsa, accompanied by rasayana chikitsa, to achieve shuddha garbha sambhava samagri (pure factors of fertilization & conception). Treatment plan was successful with intra uterine pregnancy and she has delivered a healthy female baby through caesarian section.
INTRODUCTION
According to the World Health Organization (WHO), infertility can be described as the inability to become pregnant, maintain a pregnancy, or carry a pregnancy to live birth.(1) A clinical definition of infertility by the WHO and ICMART is “a disease of the reproductive system defined by the failure to achieve a clinical pregnancy after 12 months or more of regular unprotected sexual intercourse.” (2) Infertility can further be broken down into primary and secondary infertility. Primary infertility refers to the inability to give birth either because of not being able to become pregnant, or carry a child to live birth, which may include miscarriage or a stillborn child. (3)(4)
PCOS – Poly Cystic Ovarian Syndrome is a set of symptoms due to elevated androgens (male hormones) in females.(5)(6) Signs and symptoms of PCOS include irregular or no menstrual periods, heavy periods, excess body and facial hair, acne, pelvic pain, difficulty getting pregnant, and patches of thick, darker, mood disorders, velvety skin.(7)
PCOS is the most common endocrine disorder among women between the ages of 18 and 44.(8) It affects approximately 2% to 20% of this age group depending on how it is defined.(9)(10) When someone is infertile due to lack of ovulation, PCOS is the most common cause.(5)
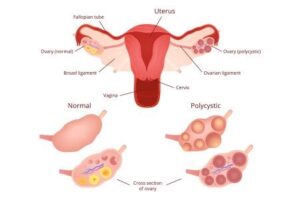
PCOS is due to a combination of genetic and environmental factors .(11)(12)(13) Risk factors include obesity, a lack of physical exercise, and a family history of someone with the condition.(14) Diagnosis is based on two of the following three findings: no ovulation, high androgen levels, and ovarian cysts.(15) Cysts may be detectable by ultrasound.(16)
Figure of pcod
PCOS has no cure.(17) Treatment may involve lifestyle changes such as weight loss and exercise.(18)(19) Birth control pills may help with improving the regularity of periods, excess hair growth, and acne.(20) Metformin and anti-androgens may also help.(20) Other typical acne treatments and hair removal techniques may be used.(20) Efforts to improve fertility include weight loss, clomiphene, or metformin.(21) In vitro fertilization is used by some in whom other measures are not effective.(21)
Ectopic pregnancy is a complication of pregnancy in which the embryo attaches outside the uterus.(22).
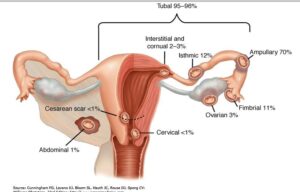
Causes of tubal pregnancy
Any sexually active woman of childbearing age is at risk of an ectopic pregnancy and often the reason for the ectopic pregnancy will never be determined. Tubal pregnancy is when the egg is implanted in the fallopian tubes. Hair-like cilia located on the internal surface of the fallopian tubes carry the fertilized egg to the uterus. Fallopian cilia are sometimes seen in reduced numbers subsequent to an ectopic pregnancy, leading to a hypothesis that cilia damage in the fallopian tubes is likely to lead to an ectopic pregnancy.(23) Women who smoke have a higher chance of an ectopic pregnancy in the fallopian tubes. Smoking leads to risk factors of damaging and killing cilia.(23) As cilia degenerate, the amount of time it takes for the fertilized egg to reach the uterus will increase. The fertilized egg, if it doesn’t reach the uterus in time, will hatch from the non-adhesive zona pellucida and implant itself inside the fallopian tube, thus causing the pregnancy.(23) Women with pelvic inflammatory disease (PID) have a high occurrence of ectopic pregnancy.(24) This results from the build-up of scar tissue in the fallopian tubes, causing damage to cilia (25). If however both tubes were completely blocked, so that sperm and egg were physically unable to meet, then fertilization of the egg would naturally be impossible, and neither normal pregnancy nor ectopic pregnancy could occur.(25)
A history of a tubal pregnancy increases the risk of future occurrences to about 10%.(25) This risk is not reduced by removing the affected tube, even if the other tube appears normal. Fertility following ectopic pregnancy depends upon several factors, the most important of which is a prior history of infertility.
CASE PRESENTATION
A lady with married life of 6yrs from Bidadi in Banglore, presented with amenorrhoea -1 & ½ month, with history of irregular, scanty, painful menstruation. Her past medical history revealed twice tubal ectopic pregnancy.
Timeline
Lady had developed irregular, scanty, painful menstruation after undergoing IVF (In-Vitro-Fertilization) in one of the Hospital at Banglore in 2017. However, IVF was not successful. Ultra-sonography of the abdomen & pelvis revealed bilateral PCOD (Poly Cystic Ovarian Disease). She was treated with oral hormonal pills for 6moths. During the course of oral hormonal treatment she had regular but painful menstruation. But she did not conceive. Later she visited Ayurveda clinic in Mysore for her problems. Later in June 2018 she consulted our hospital. She underwent ultra-sonography of abdomen & pelvis (August 2018). This report also revealed as bilateral PCOD.
In 2013, she had undergone emergency laparoscopic right sided salpingectomy under spinal anaesthesia, as she was diagnosed very late with right sided ruptured tubal ectopic pregnancy.
In 2015, she had conceived second time, however, again it was left tubal pregnancy, as it was diagnosed early at 5wks, it was terminated by oral pills & was treated with medicine Methotrixate.
After that she underwent HSG (Hystero-Salpingography) & the report showed,
Left tube –hydrosalpinx in ampullary region, fimbrial end clumped. However, free spill was seen.
After this event she did not conceive.
In 2017, once she underwent IVF (In-Vitro-Fertilization) in Milan Hospital Banglore. However, it was not successful. Since then she developed irregular menstruation & diagnosed with PCOD (Poly Cystic Ovarian Disease) in ultrasonography report.
In June 2018, she came to SDM Institute of Ayurveda & Hospital Banglore. From august 2018 she was regular in taking medicine and councelling.
Menstruation was found to be irregular (50- 90 days usually gets after taking hormonal pills she used to get her menstruation), scanty, painful, 3 – 4 days -dark blackish red, more clots than liquid bleeding & required 1 pad/day, but she changed 2pads/day to maintain hygiene. Her inner garment used to get stained during menstruation.
Diagnostic focus and Assessment
Per Vaginal Examination revealed – Uterus- AVNS, vagina was bathed in yellowish – white discharge.
Per Speculum Examination revealed – Cervical erosions all over the cervix with severe yellowish- white discharge adhered to the cervix & vagina.
HSG (Hystero-Salpingography) in 2015 – Left tube –hydrosalpinx in ampullary region, fimbrial end clumped. However, free spill was seen.
After analyzing, with the ayurvedic principles, it was diagnosed as,
‘Vandhyatva’ ‘Secondary Infertility’ due to PCOS ( PCOD, Pimples, Hair loss)
In this case, the six causative factors (Ashuddha garbha sambhava samagri (impure factors of fertilization & conception) & manasika shalyas ) for vandhyatva are explained as follows,
- Beeja dushti – Anovulation due to PCOD,
- Rutu dushti – Irregular menstrual cycle,
- Kshetra dushti – Hydrosalpinx in the ampullary region of the left fallopian tube, right sided – salpingectomy done, cervical erosion.
- Arthava dushti (Arthavakshaya,Athyarthava,Kashtarthava) – irregular menstruation, sometimes amenorhoea and other time meno-metrorrhgia/oligomenorrhoea, dysmenorrhoea.
- Ambu dushti – Body fluids -All the doshas vitiated (in bhedhavastha of shad kriyakala) and ama (free radicals) produced also vitiates body fluids. Her vyadhi kshamatva (immunity) decreased (often she gets rhinitis, cough). Homeostasis was disturbed in the body.
- Shalyas – Stressful factors (manaha shareera bhadhakarani iti shalyani.) were present in her. As she was, physically, mentally, emotionally & socially stressed out, due to medical history. This leads to disturbance in homeostasis. Lady had entered into flight mode due to stress.
Therapeutic focus and Assessment
Chikitsa was aimed at objectives ‘A’ and ‘B’
Objectives ‘A’
- Ashuddh garbha sambhava samagri – impure factors of fertilization & conception-rutu (ovulation & menstruation), kshetra (female reproductive system), ambu (body fluids), beeja (ovum, sperm & zygote), in order to achieve shuddha garbha sambhava samagri (pure factors of fertilization & conception).
- Arthava dushti irregular menstruation, sometimes amenorhoea and other time meno-metrorrhgia/oligomenorrhoea, dysmenorrhoea, in order to achieve shuddha arthava (purity & alignment in menstrual cycle & endocrinal co-ordination).
- Shalyas -Physical, Mental, Emotional & social Stressful factors, in order to attain prassannatmendriya mana (satiation of body, mind & spiritual).
Objectives ‘B’
- To attain health in mother at all levels (physical, mental, emotional, spiritual and social).
- To obtain healthy progeny.
The chikitsa (treatment) schedule planned as below,
Deepana Pachana chikitsa – digestive & assimilative medicine-is given prior to shodhana chikitsa.
Shodhana chikitsa – detoxification treatment
Virechana karma (detoxification- Medical purgation treatment),
Sarvanga Abhyanga & Swedana (medicated oil massage & steam).
Kala basthi karma (medicated enema),
Nasya karma (medicated nasal drops),
Uttara basthi (medicated intra-uterine treatment),
Music therapy councelling and yoga – mohana raga, surya namaskara, chinmudra pranayama & meditation, omkara recitation
Oral medicines
For cervical erosion –
Sthanika chikitsa per-vaginal treatment as follows,
Yoni prakshalana- medicated vaginal wash (vaginal douch)
Yoni dhoopana – medicated vaginal fumigation
Yoni pichchu dharana- medicted vaginal tampoon
Regular councelling was planned as per the changes & feedback from the lady and her husband.
The treatments were carried out as scheduled in the Table 1,2,3,4.
TREATMENT SCHEDULED.
From August 2018 to October 2018
Deepana – Pachana was done with Tablet Trikatu 1-1-1 continuously for 6months.
Councelling was done daily 1hour for 10 days, then once in week for 1month- 1hr, followed by once in a week for 1month-15min.
Yoga –Surya namaskara 6times 5days in a week, Chinmudra pranayam, Meditation & Omkara recitation for 15min twice daily.
Music therapy – Mohan raga music was done for 2hours, once in a week for 3months.
Prayer –Universal Prayer shloka was given in writing & advised to recite twice daily accompanied by her husband.
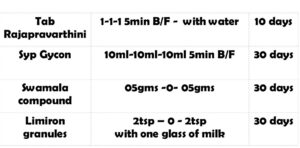
Table 1 Oral medicine
From last week of October 2018 to first week of November 2018
Table 2 Virechana karma Sthanika chikitsa Sarvadaihika chikitsa
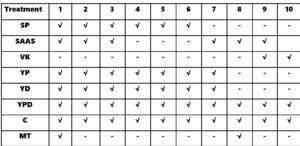
SP-Sneha Pana, SAAS-Sarvanga abhyanga and swedana, VK-Virechana karma, YP-Yoni prakshalana, YD – Yoni dhoopana, YPD – Yoni pichchu dharana, C – Councelling, Music therapy.
From last week of November 2018 to first week of December 2018
Table 3 Kala Basthi karma Sarvadaihika chikitsa

ABK – Anuvasana Basthi Karma, NBK – Niruha Basthi Karma, SAAS-Sarvanga abhyanga and swedana, SN – Surya Namaskara, CM – Chin Mudra, MT – Music Therapy, C – Councelling.
In first week of January 2019
Table 4 Nasya karma chikitsa

MNK – Marsha Nasya Karma, C – Councelling, MT – Music Therapy
RESULTS
After the virechana karma followed by kala basthi, she had her menstruation on 28/12/2018 (after 6 months of amenorrhoea). Menstruation was uneventful, that is she did not suffer with any pains and liquid part was more than the clots in menstrual bleeding. Color of menstrual bleeding was light blackish red. Her inner garments were not stained. 5 Days bleeding with less small clots was observed by the patient. Her weight also increased by 2kg after the kala basthi (from 58kg to 60kg). By this time, pimples had reduced completely. She was happy as her face was clear & chubby cheeks.
After the sthanika chikitsa (local per-vaginal treatment) through vaginal route, cervical erosion healed and healthy cervix noted.
The two follow up examination showed- P/V- uterus –AVNS, no white discharge was seen. P/S- Cx –healthy.
She missed her menstruation on 28thJanuary 2019. On 22nd February 2019 urine test for pregnancy was positive.
It was confirmed as intra-uterine pregnancy with gestation sac & yolk sac, in ultra-sonography of abdomen & pelvis.
Repeat scan was done on 14/03/19 which showed CRL-1.95cm, yolk sac was seen, fetal heart pulsation seen 178beats/min. Intra-uterine pregnancy of 8wks 4days.
Discussion:
Discussion is a detailed treatment of a topic in speech or writing, in order to reach a decision or to exchange ideas. Herewith I have tried to analyse the ayurvedic samprapthi & treatments for the infertility due to PCOS & ectopic pregnancy, with the help of our proud Acharya’s principles.
It has been explained in our samhitas, the purity of arthava (menstrual flow) is the primary unit for garbhotpatti (fertilization & conception). Our acharyas have highlighted that the menstrual blood does not leave any stain on the cloth. (26) This is the sign of purity in menstrual blood & indicates the forthcoming ovulation.
It was noted that, after course of deepana, pachana,virechana karma & kala basthi karma, menstruation was uneventful, that is she did not suffer with any pains and liquid part was more than the clots in menstrual bleeding. Color of menstrual bleeding was light blackish red. Her inner garments were not stained. 5 Days bleeding with less small clots was observed by the patient. This indicates the purity of the arthava menstrual bleeding.
Her weight also increased by 2kg after the kala basthi (from 58kg to 60kg). By this time, pimples had reduced completely. She was happy as her face was clear & chubby cheeks.
In Charaka Samhita Shareera Sthana 4th chapter named Mahati garbhavakranthi, commentator of Charaka Samhitha, Acharya Chakrapani has explained that, garbha gradually enters garbhashaya. However, if there is vikara in garbha, by the time it reaches kukshi or garbhashaya, it may get destroyed (kukshau jayamana; kukshau vinasham prapnoti) & brings in death (katsnyernavinashyan iti marana gachchan) (27).
Our Acharyas have written in sutra form. While explaining the early growth of fertilized ovum, Acharya Charaka has used the term kheta bhuta which means shleshma sadrashya- slippery in nature(28), which is quiet similar to Zona pellucida-outer layer of the zygote. This layer helps the zygote, to slide down with its slippery nature, from fallopian tube to the intra-uterine cavity of the uterus for the implantation. One of the etiological factors for the tubal pregnancy is pre-mature loss of the layer zona-pellucida, loss of kheta bhuta can be compared to sthanika shleshma ksheena, when the fertilized ovum is in the ampulla part of the fallopian tube, as the fertilization occurs in the ampulla. Thus the zygote gets fixed to the fallopian tube, leading to rupture of the tube & destruction of the zygote if goes unnoticed by the medical faculty. Thus tubal pregnancy gets destroyed & increases the mortality rate of the mother.
Subserosa layer of the fallopian tube is composed of loose adventitious tissue, blood vessels, lymphatics, an outer longitudinal and inner circular smooth muscle coats. This layer is responsible for the peristaltic action of the fallopian tubes. In turn this peristaltic movement helps in the gliding movements of zygote towards the intra-uterine cavity of the uterus. These movements can be compared to apana-vata, which is present in shroni pradesh & is responsible for all the movements in the shroni. There is apana vata vigunata (improper function of apana vata). This is exhibited in the form of, irregular menstruation, sometimes meno-metrorragia other time oligomenorrhoea, dysmenorrhoea.
The inner layer of fallopian tube is a single layer of simple columnar epithelium. The columnar cells have microscopic hair-like filaments (cilia) predominantly throughout the tube, but are most numerous in the infundibulum and ampulla. Estrogen increases the production of cilia on these cells. Between the ciliated cells are peg cells, which contain apical granules and produce the tubular fluid. This fluid contains nutrients for spermatozoa, oocytes, and zygotes. This can be compared to shleshma, rasadhatu. Tubal fluid flows against the action of the cilia, toward the fimbrial end. The fertilized ovum, now a zygote, travels towards the uterus aided by activity of tubal cilia and activity of the tubal muscle. Again these movements are responsibility of apana-vata.
The early embryo requires critical development in the fallopian tube. After about five days the new embryo enters the uterine cavity and on about the sixth day implants on the wall of the uterus, which is again co-ordinate activity of vata-kapha-pitta in shroni & minute srotas in shroni.
Fallopian tube obstruction is associated with infertility and ectopic pregnancy. Risk factors for ectopic pregnancy include: pelvic inflammatory disease, often due to chlamydia infection, tobacco smoking, prior tubal surgery, a history of infertility, and the use of assisted reproductive technology. Those who have previously had an ectopic pregnancy are at much higher risk of having another one. Most ectopic pregnancies (90%) occur in the fallopian tube, which are known as tubal pregnancies (29).
Presence of multiple pimples, heavy perspiration in palms and soles, often suffering from cold, constipation, irregular menstruation (more often amenorrhoea), anxiety and depression indicates the reduced immunity, accumulation of free-radicals in the body, disturbances at mental, emotional, spiritual and social levels due to loss of zygote in twice ectopic tubal pregnancies and unsuccessful IVF.
Our acharyas have highlighted the importance of shuddh garbha sambhava samagri (pure sperm, ovum, uterus and bod fluids) to obtain a healthy garbha. And shuddhata of shareera & manas (pure body & mind) is also equally important.
Acharya Sushruta while explaining swastha laxana, has given equal importance to equilibrium at physical level-shareera (samadhosha, samagni, samadhatu, sama mala & kriyas of dosha-agni-dhatu-mala), spiritual level -prasannata of atma (satiation or brahmananda), mental level -prasannata of mana (happiness in all situations), emotional level -prasannata of indriyas (liveliness jnyanendriyas & karmendriyas).
In jathaharini adhyaya, it has been mentioned that, to get a healthy progeny, the couple have to follow ‘Dharma palana ( Dharanath dharmaha)’that is good conduct to maintain health at physical, mental, emotional, spiritual and social levels.
By considering the above mentioned etiological factors, the exclusive treatment schedule was planned to target health at physical, mental, emotional, spiritual and social level. The plan is shown in the following table 5.
Table 5 Treatment plan

After the Deepana Pachana for 2months, virechana karma was done after the samyak snigdha laxana with trivruth leha & gandharva hasthadi taila respectively on 9th & 10th day.
On 15th day follow up after the virechana karma, her pimples had subsided. Sweating in palms and soles had reduced completely. Sneezing, running nose, cold had been subsided completely. Up to 1month same health was maintained.
In second course, kala basthi karma as follows,
Anuvasana basthi- was done with Phala ghrita 75ml- for 9 days. On 6th 12th day of kala basthi karma, Gandharva hasthadi taila 50 ml- for 2days was used for Anuvasana basthi karma.
Niruha basthi- was done with Honey 50ml+ Saindhava lavana10gms+ Shatapushpa churna10gms+ Phala ghrita75ml+ Eranda mula churna kashaya-300ml-for 5days.
After the completion of kala basthi karma, lady had her menstruation (after 6months of amenorrhoea) on 28th December 2018. Lady reported that, her menstruation was uneventful, without any pains. Consistency wise liquid part was more than the clots in menstrual bleeding. The colour of menstrual bleeding was light blackish red. 5 Days bleeding with less small clots was observed by the patient. 3pads/day changed by the lady. Arthava (menstrual bleeding) highlights about homeostasis in the body, as arthava is the upadhatu (sub-part) of rasa dhatu. Homeostasis was attained. It also indicates the forthcoming ovulation.
Activeness, good healthy raport with family and friends, involvement in her daily chores and smiling face throughout the day in lady (observed by her husband, friend and in follow up check-up). This indicates the stress free body, mind, emotions, spiritual and social well being in lady. Music therapy, surya namaskara, chinmudra pranayama are the parts of rasayana chikitsa. They have succeeded in returning her regular dinacharya. Music and yoga are the part and parcel of our daily work. For manasika shalya harsha chikitsa is indicated.
From 8th day of menstruation that is on 5th January 2019, marsha nasya karma was started with anu-taila. The nasya treatment was done up to 11th January 2019. Councelling and music therapy were carried out on 5th and 11th January 2019.
She missed her menstruation in January 2019. On 22nd February 2019 urine test for pregnancy was done at home by patient herself, which was positive for pregnancy. It was confirmed as intra-uterine pregnancy with gestation sac & yolk sac, in ultra-sonography of abdomen & pelvis.
Repeat scan was done on 14/03/19 which showed CRL-1.95cm, yolk sac was seen, fetal heart pulsation seen 178beats/min. Intra-uterine pregnancy of 8wks 4days.
Patient consent:
Informed consent regarding documentation and publication of the case study was obtained from the lady & her husband. Her husband has written about this case in review column in SDMIAH.
Conclusion:
Quality of life was hampered in lady due to irregularity in consuming food, sleep pattern, stress in day today life.
Emotional stress had taken over her completely. Hampered quality life had negative effect on shuddha garbha sambhava samagri, leading to ashuddha garbha sambhava samagri (impure factors of fertilization), irregular menstrual cycles & irregular flow, scanty flow.
She was unable to conceive child. She had history of bilateral ectopic tubal pregnancy & losing one tube in salpingectomy and the other tube with hydrosalpinx.
Ayuveda has played very impotant role through dinacharya, virechana karma, kala basthi and marsha nasya karma, music therapy, yoga and pranayama, in obtaining shuddha garbha sambhava samagri (pure factors of fertilization) in the form of delivering a healthy female child through elective caesarian section. The aim and objects which was planned before starting the treatment, has been reached successfully.
So, the term has been used as ‘tapas by the couple’ to get a healthy child.
So the saying ‘Child by choice & not by chance’ should be taught to our people.
Aviruddhe Dhruvam Daive Kale Yukthasya Karmanaha.
Financial support & sponsorship
Lady and her husband have taken care of financial situation. No other support or sponsorship was given for this case throughout the treatment courses.
Conflicts of Interest
Author has no competing interest, as this case study was done with exclusive interest to make the lady to conceive naturally and healthy progeny.
SARVESHAM AROGYAM BHAVATU

Dr. Bharathi D. Anvekar BAMS, MS, PhD
Professor and Consultant,
Dept of Shalya tantra, Prasuthi Tantra & Stree-Roga
S. D. M. Institute of Ayurveda & Hospital,
Banglore-74 Ph:080-22718025 Mob:98864 10690
For Health videos visit healthvision
REFERENCES
- World Health Organization 2013. “Health Topics: Infertility”. Available http://www.who.int/topics/infertility/en/. Retrieved November 5, 2013.
- Zegers-Hochschild F.; Adamson G.D.; de Mouzon J.; Ishihara O.; Mansour R.; Nygren K.; Sullivan E.; van der Poel S. (2009). “The International Committee for Monitoring Assisted Reproductive Technology (ICMART) and the World Health Organization (WHO) Revised Glossary on ART Terminology, 2009”. Human Reproduction. 24 (11): 2683–2687. doi:10.1093/humrep/dep343. PMID 19801627.
- World Health Organization 2013.”Sexual and reproductive health: Infertility definitions and terminology”. Available http://www.who.int/reproductivehealth/topics/infertility/definitions/en/. Retrieved November 5, 2013.
- Rutstein, Shea O., and Iqbal H. Shah. “Infecundity, Infertility, and Childlessness in Developing Countries.” DHS Comparative Reports No. 9 (2004): 1-57.
- “Polycystic Ovary Syndrome (PCOS): Condition Information”. National Institute of Child Health and Human Development. January 31, 2017. Retrieved 19 November 2018.
- “Polycystic ovary syndrome (PCOS) fact sheet”. Women’s Health. December 23, 2014. Archived from the original on 12 August 2016. Retrieved 11 August 2016.
- “What are the symptoms of PCOS?” (05/23/2013). National Institute of Child Health and Human Development (NICHD). Archived from the original on 3 March 2015. Retrieved 13 March 2015.
- Teede H, Deeks A, Moran L (2010). “Polycystic ovary syndrome: a complex condition with psychological, reproductive and metabolic manifestations that impacts on health across the lifespan”. BMC Med. 8 (1): 41. doi:10.1186/1741-7015-8-41. PMC 2909929. PMID 20591140.
- “How many people are affected or at risk for PCOS?”. Eunice Kennedy Shriver National Institute of Child Health and Human Development. 2013-05-23. Archived from the original on 4 March 2015. Retrieved 13 March 2015.
- Editor, Lubna Pal (2013). “Diagnostic Criteria and Epidemiology of PCOS”. Polycystic Ovary Syndrome Current and Emerging Concepts. Dordrecht: Springer. p. 7. ISBN 9781461483946. Archived from the original on 2017-09-10.
- De Leo V, Musacchio MC, Cappelli V, Massaro MG, Morgante G, Petraglia F (2016). “Genetic, hormonal and metabolic aspects of PCOS: an update”. Reproductive Biology and Endocrinology (Review). 14 (1): 38. doi:10.1186/s12958-016-0173-x. PMC 4947298. PMID 27423183.
- ^ Jump up to:a b c d e Diamanti-Kandarakis E, Kandarakis H (2006). “The role of genes and environment in the etiology of PCOS”. Endocrine. 30 (1): 19–26. doi:10.1385/ENDO:30:1:19. PMID 17185788.
- Dumesic DA, Oberfield SE, Stener-Victorin E, Marshall JC, Laven JS, Legro RS (2015). “Scientific Statement on the Diagnostic Criteria, Epidemiology, Pathophysiology, and Molecular Genetics of Polycystic Ovary Syndrome”. Endocrine Reviews (Review). 36 (5): 487–525. doi:10.1210/er.2015-1018. PMC 4591526. PMID 26426951.
- “How many people are affected or at risk for PCOS?”. Eunice Kennedy Shriver National Institute of Child Health and Human Development. 2013-05-23. Archived from the original on 4 March 2015. Retrieved 13 March 2015.
- “Polycystic Ovary Syndrome (PCOS): Condition Information”. National Institute of Child Health and Human Development. January 31, 2017. Retrieved 19 November 2018.
- “How do health care providers diagnose PCOS?”. Eunice Kennedy Shriver National Institute of Child Health and Human Development. 2013-05-23. Archived from the original on 2 April 2015. Retrieved 13 March 2015.
- “Is there a cure for PCOS?”. US Department of Health and Human Services, National Institutes of Health. 2013-05-23. Archived from the original on 5 April 2015. Retrieved 13 March 2015.
- Mortada R, Williams T (2015). “Metabolic Syndrome: Polycystic Ovary Syndrome”. FP Essentials (Review). 435: 30–42. PMID 26280343.
- ^ Jump up to:a b Giallauria F, Palomba S, Vigorito C, Tafuri MG, Colao A, Lombardi G, Orio F (2009). “Androgens in polycystic ovary syndrome: the role of exercise and diet”. Seminars in Reproductive Medicine (Review). 27 (4): 306–15. doi:10.1055/s-0029-1225258. PMID 19530064.
- National Institutes of Health (NIH) (2014-07-14). “Treatments to Relieve Symptoms of PCOS”. Archived from the original on 2 April 2015. Retrieved 13 March 2015.
- National Institutes of Health (NIH) (2014-07-14). “Treatments for Infertility Resulting from PCOS”. Archived from the original on 2 April 2015. Retrieved 13 March 2015.
- Kirk E, Bottomley C, Bourne T (2014). “Diagnosing ectopic pregnancy and current concepts in the management of pregnancy of unknown location”. Human Reproduction Update. 20 (2): 250–61. doi:10.1093/humupd/dmt047. PMID 24101604.
- Lyons RA, Saridogan E, Djahanbakhch O (2006). “The reproductive significance of human Fallopian tube cilia”. Human Reproduction Update. 12 (4): 363–72. doi:10.1093/humupd/dml012. PMID 16565155.
- Tay JI, Moore J, Walker JJ (2000). “Ectopic pregnancy”. Western Journal of Medicine. 173 (2): 131–4. doi:10.1136/ewjm.173.2.131. PMC 1071024. PMID 10924442.
- ^ Jump up to:a b c d Speroff L, Glass RH, Kase NG (1999). Clinical Gynecological Endocrinology and Infertility, 6th Ed. Lippincott Williams & Wilkins (1999). p. 1149ff. ISBN 978-0-683-30379-7.
- शुक्रशोणितशुद्धिशारीरं तत्र शुक्रशोणितयोः शुद्धयोरेव शुद्धिर्दुष्टदोषासम्पर्कता||१-२|| यदार्तवं वासः- स्थितं शुष्कमुदकप्रक्षालितं वासो न विरञ्जयेत् रागोपेतं वस्त्रं न कुर्यात् तत् प्रशंसन्ति, ‘गर्भजननाय’ इति शेषः||१७||
- शारीरस्थानम् – २. शुक्रशोणितशुद्धिशारीरम् निबन्धसङ्ग्रह व्याख्या (डल्हण कृत )
- Charaka samhitha shareera sthana 4th chapter kukshau jayamana; kukshau vinasham prapnoti) & brings in death (katsnyernavinashyan iti marana gachchan) यतश्च जायमानःकुक्षौ विनाशं प्राप्नोति, यतश्च कार्त्स्न्येनाविनश्यन् विकृतिमापद्यते, तदनुव्याख्यास्यामः||३||
- स सर्वगुणवान् गर्भत्वमापन्नः प्रथमे मासि सम्मूर्च्छितः सर्वधातुकलुषीकृतः खेटभूतो भवत्यव्यक्तविग्रहः सदसद्भूताङ्गावयवः||९|| खेटः श्लेष्मा; तेन खेटभूत इति श्लेष्मसदृश इत्यर्थः
- Cecchino GN, Araujo Júnior E, Elito Júnior J (September 2014). “Methotrexate for ectopic pregnancy: when and how”. Archives of Gynecology and Obstetrics. 290 (3): 417–23. doi:10.1007/s00404-014-3266-9. PMID 24791968.